
The contribution of patients and patient experts provides tangible value to other stakeholders and society that should be fairly compensated. Currently, there is no transparent and consistent system for financial compensation in place that reflects the level of individual contribution and expertise.
Compensation in this context means honoraria or other financial compensation by third parties (no patient organisations) to patient advocates for individual tasks such as advisory boards, doing presentations, providing substantial feedback, reviewing complex documents etc. Reimbursement of travel cost, daily allowances for expenses etc. do not count as financial compensation for tasks.
What are covering here?
- Why is Fair Market Value an issue for patient advocates?
- What are the unresolved challenges in applying Fair Market Value to the work of patient advocates today?
- What can we draw on to develop a Fair Market Value model?
- Results of the WECAN Fair Market Value Survey (2018)
- What’s next?
- Members of the WECAN Fair Market Value Workgroup
Why is „fair market value“ an issue for patient advocates?
Patient advocates are mission-driven, but some individuals need to make their living – and in any case it should be their own choice to volunteer or not. If patient advocates are staff members, their organisations still need to have (and pay for) more staff if contributing to an increasing number of stakeholder meetings. Patient advocates are often the only unpaid/poorly paid experts in the room.
Financial compensation for patients should be offered at meetings of industry/regulators/other stakeholders for…
- advisory and collaborative roles (“patient input”)
- consultancy work (e.g. support the creation of services)
- speaker roles at internal meetings
- speaker roles at external events and conferences
Financial compensation should be considered not only by industry, but also by governmental committees or commercial conference organizers.
What are the unresolved challenges in applying Fair Market Value to the work of patient advocates today?
- Industry is nervous about perception of bribery, but criteria applied to address these vary widely
- Patient experience and expertise not valued in the same way as other professionals
- Frequently patient advocates are offered no compensation (their “networking” or “having a voice” is already seen as “return on invest”)
- Fair market value rates rarely differentiate between patients just with individual disease experience vs. highly trained, experienced patient experts who have invested huge amounts of time in building knowledge, evidence and contributions
- Preparation time and travel time invested for meetings often disregarded
- Inconsistency of methodologies across companies (in rates, engagement time, travel time)
- Huge variance in rates often leads to the least common denominator, providing wrong incentives and disincentives to contribute
- Often no choice who receives the compensation (to individual or to organisation)
- Sometimes not even a right to refuse compensation (opt out), if the organisation’s policy does not allow to receive honoraria
A fair, systematic and structured approach to fair market value is needed:
- Both patient organisations and industry see the need for a fair, systematic and structured approach to compensation to patients, representing fair market value:
- Evaluation of fair market value could be done e.g. on
- individual experience/expertise (e.g. years of experience, prior training, involvement in scientific meetings, transferable skills)
- level of contribution
- complexity of tasks delivered (pure participation, small tasks, trainer/reporter, specialist/expert level)
- total time invested (preparation, presence and follow-up time, travel time)
What we can draw on to develop a Fair Market Value model…
- EUPATI Guidance’s definition of patients
When everyone refers to “patient input”,
EUPATI has developed guidance documents on patient engagement (chapter 5, “Defining Patient”) which also describes different roles patients can take on when engaging with stakeholders:
“Individual patients” / “carers”: personal experience of living with disease
“Patient Advocates”: insight & experience in larger population of patients
“Patient Organisation Representatives”: expressing the collective views of a patient organisation
“Patient Experts”: in addition to disease-specific expertise, have the technical knowledge in R&D and/or regulatory affairs - WECAN’s “Guiding Principles on Reasonable Legal Agreements between Patient Advocates and the Pharmaceutical Industry”
Chapter 8 of the Guiding Principles, developed by WECAN in partnership with PFMD and 12 pharmaceutical companies and released in October 2018 based on the data from the WECAN FMV Survey, provides the rationale, example and guiding principles on a fair compensation of patient advocates. It stipulates that “honorarium or financial compensation for services should take into account individual expertise and training, total amount of time invested, complexity of tasks, country of origin, and other contributing factors, similar to compensation of other highly trained professionals or consultants”. - EATG’s tool which stratifies compensation in accordance with the complexity of tasks delivered by the patient advocate
1 – work group participation
2 – small tasks- e.g protocol revisions
3 – intermediate level, e.g. trainer, report work
4 – specialist/expert level
Results of the WECAN Fair Market Value Survey (2018)
In order to help WECAN to formulate a contribution and recommendation in the context of the current debate about “Fair Market Value” that represents the opinion of the patient advocacy community, WECAN ran a survey between 23 July and 10 September 2018.
122 responses of patient advocates from 38 countries were received:
- 41.8% from solid cancers (n=51)
- 15.6% from non-malignant and malignant hematology (n=19)
- 9.8% from non-cancer rare diseases (n=12)
- 20.5% from other disease areas (e.g. rheumatic, psioriasis, multiple sclerosis, Parkinson’s, lung diseases like COPD and asthma, metabolic, infertility, HIV, bone diseases, n=25)
- 12.3% without specific disease focus, or disease not mentioned
68.0% of respondents the respondents said to accept financial compensation for their individual activities as patient advocate or expert, either personally or through their organization (n=83).
74.7% of those who generally accept compensation also actually received financial compensation in the past 6 months.
Brief summary of results
- Patient community strongly agrees that the individual expertise, community insight, community leadership, complexity of tasks, total time invested should increase FMV value rate
- Factors for measuring individual expertise should include specifically advocacy track record, disease and treatment knowledge, healthcare/research systems knowledge, personal skills, completion of training programmes, personal experience
- Different rates by country of residence were seen skeptical
- Patient community disagrees that factors like networking opportunities, travel, learning, prestige, visibility, access to treatments or healthcare professionals should decrease the FMV rate
- Travel time should be compensated, either full or at least partial. Only 16% think no compensation for travel time is fair.
- Right to opt out from financial compensation, and right of choice of recipient (patient organisation or patient advocate) has strong support
Detailed results
Factors that potentially increase the Fair Market Value rate
There was strong agreement on FMV differentiation based on individual expertise and training, community insight, community impact and leadership, complexity of tasks, total time invested. A strong variance in opinion whether FMV rate should be influenced by country of residence of patient advocate was observed. There was no significant difference in opinion between those that receive honoraria and those who don’t.
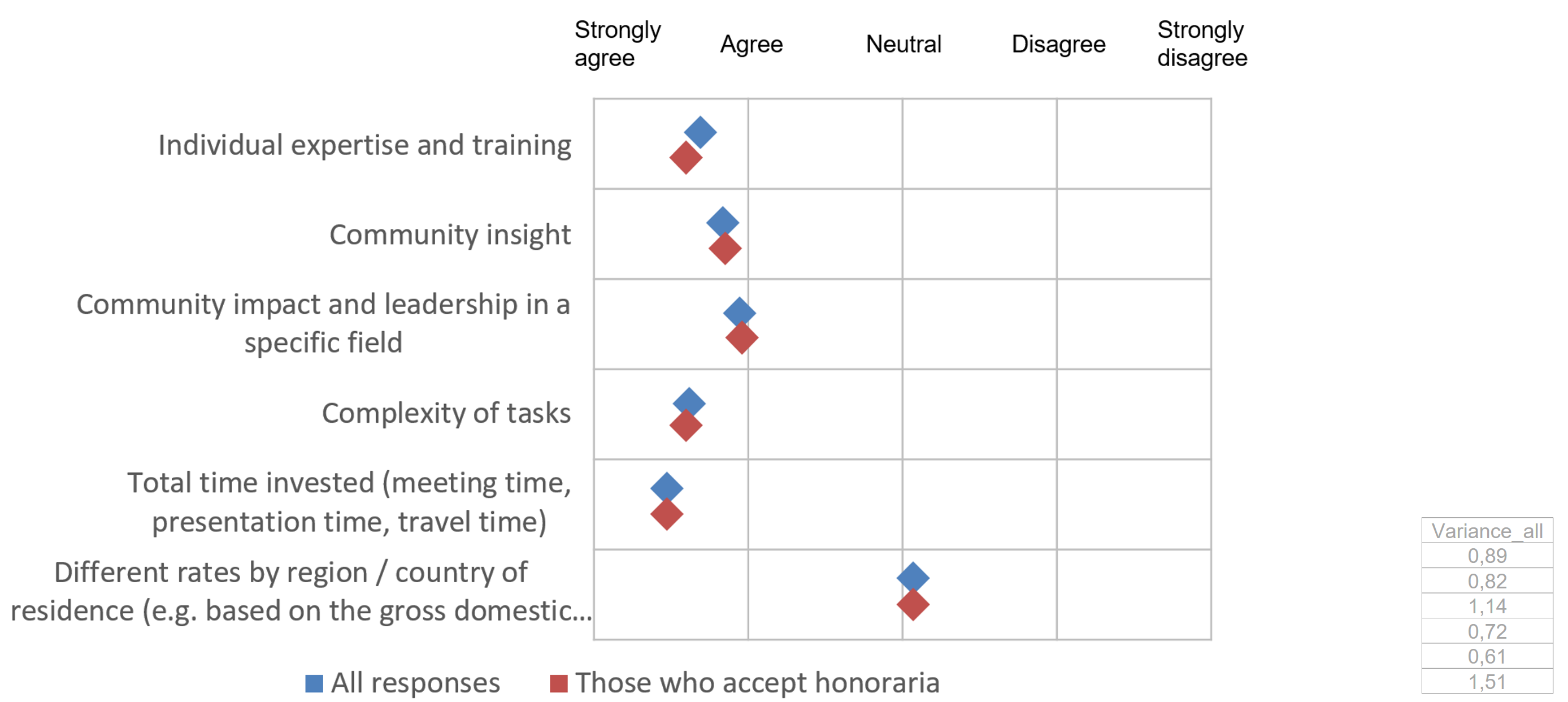
Q4: When looking at the Fair Market Value rate that patients and patient advocates receive as compensation for tasks (such as advisory boards, doing presentations, providing feedback, protocol review etc), should the following factors increase the level of your financial compensation: Rate 1-5: strongly agree, agree, neutral, disagree, strongly disagree: n=122 responses
Factors for measuring individual expertise and training
In order of priority, patient advocates agreed that factors like systems knowledge, disease knowledge, achievements / track record in advocacy, personal experience with disease, completion of training programmes and number of years in patient advocacy could be used to measure individual expertise. There was a difference in opinion between those that receive honoraria and those who don’t whether personal skills should influence the FMV rate.
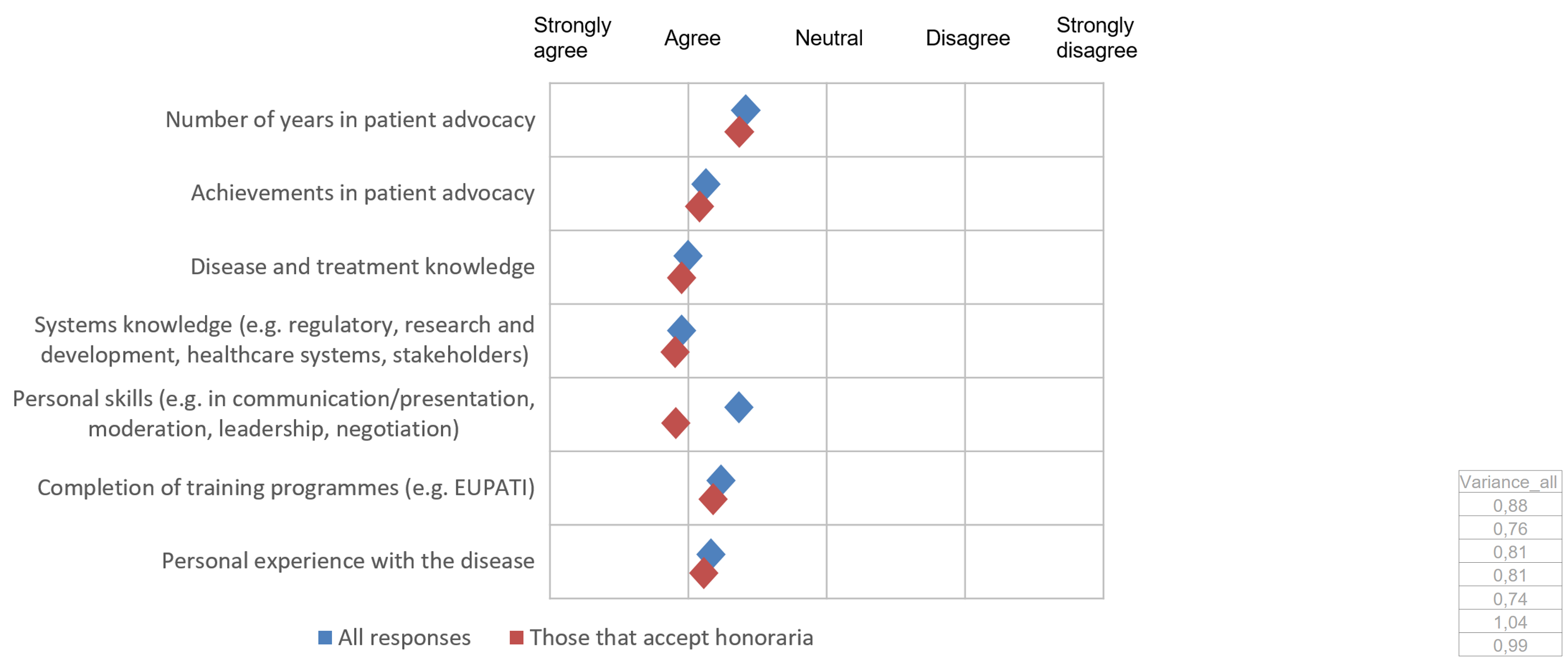
Q6: Should the following factors be used to measure individual expertise and training of a patient advocate to determine a Fair Market Value rate? Rate 1-5: strongly agree, agree, neutral, disagree, strongly disagree: n=122 responses
Factors that potentially decrease the FMV rate
Patient advocates disagreed that networking opportunities, nice locations of meetings, learning opportunities, career development opportunities, prestige and visibility or access to healthcare providers justify a reduction of FMV rates. Improving access to specific treatment for themselves or their community had lowest level of disagreement.
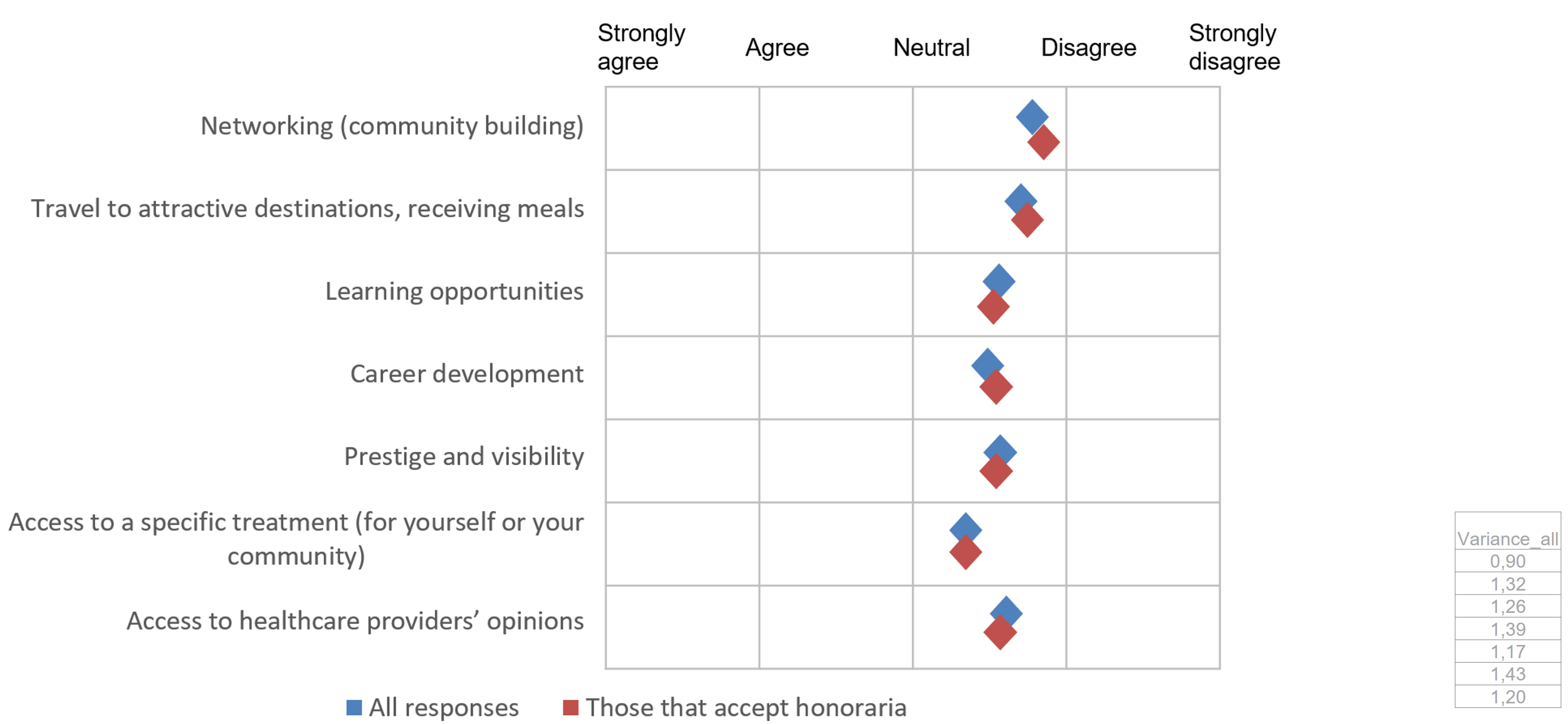
Q5: When looking at the Fair Market Value rate that patients and patient advocates receive as compensation for tasks, should the following factors decrease the level of your financial compensation? Rate 1-5: strongly agree, agree, neutral, disagree, strongly disagree: n=122 responses
Compensation for travel time
Often patients are only compensated for time present at meetings, or for the time they have active contributions during meetings, even though the meeting may cause absences of multiple days.
84.4% of patient advocates felt that it would be most fair to receive full compensation or at least partial compensation of travel time to meetings. Only 15.6% felt it is fair not to compensate travel time at all.
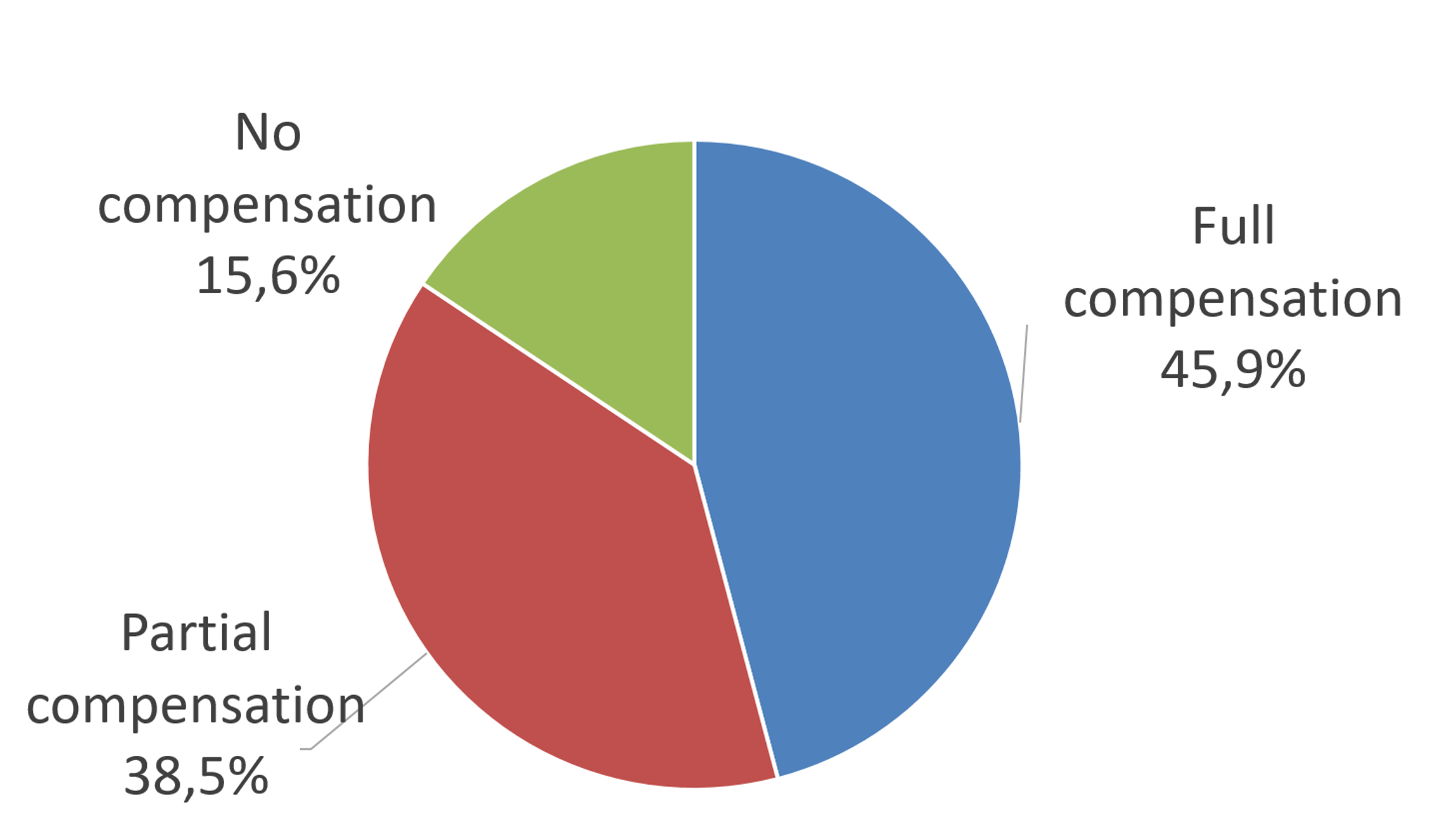
Q7: Compensation for travel time can recognize the value associated with the time a patient advocate could be spending on other things instead of travelling to and from a meeting. At the same time, requiring financial compensation for travel time may be seen as the responsibility of the individual or organization and not the client. Wherever legally allowed, which of the following options do you perceive as most fair for both the patient advocate and the meeting organizer?: n=122 responses
Opting out from compensation, or choosing the recipient
63.9% of patient advocates agrees that the “Right to opt out from any financial compensation (e.g. if codes of practice or bylaws of the organisation does not allow any compensation)” should be considered.
87.7% of patient advocates thought that the “Right of choice of recipient of payment (to the organisation, or to the patient advocate, or donation to a third party etc)” should be considered.
What’s next?
In the interests of the patient community, WECAN’s FMV workgroup is actively driving the current debate on fair compensation of patient advocates forward, based on the results of the data from WECAN’s FMV survey and WECAN’s Guiding Principles on Legal Agreements. For example, WECAN contributes to ongoing FMV discussions in the EFPIA Patient Think Tank, the IMI PARADIGM project, and in multi-stakeholder discussions in Patient Focused Medicines Development (PFMD).
Members of the WECAN Fair Market Value Workgroup
The following patient advocates are members of the WECAN FMV workgroup: Jan Geissler, Ananda Plate, Gilliosa Spurrier, Judith Taylor, Kathy Oliver, Gordon Oliver, Susanna Leto
For download:
Summary presentation of WECAN Fair Market Value Survey (PDF, 28 Oct 2019)